


For your consideration. Read the research below, or download the document:
Masks Don’t Work
A review of science relevant to COVID-19 social policy
Denis G. Rancourt, PhD
Researcher, Ontario Civil Liberties Association (ocla.ca)
Working report, published at Research Gate
(https://www.researchgate.net/profile/D_Rancourt)
April 2020
Summary / Abstract
Masks and respirators do not work.
There have been extensive randomized controlled trial (RCT) studies, and meta-analysis reviews of RCT studies, which all show that masks and respirators do not work to prevent respiratory influenza-like illnesses, or respiratory illnesses believed to be transmitted by droplets and aerosol particles.
Furthermore, the relevant known physics and biology, which I review, are such that masks and respirators should not work. It would be a paradox if masks and respirators worked, given what we know about viral respiratory diseases: The main transmission path is long-residence-time aerosol particles (< 2.5 μm), which are too fine to be blocked, and the minimum-infective-dose is smaller than one aerosol particle.
The present paper about masks illustrates the degree to which governments, the mainstream media, and institutional propagandists can decide to operate in a science vacuum, or select only incomplete science that serves their interests. Such recklessness is also certainly the case with the current global lockdown of over 1 billion people, an unprecedented experiment in medical and political history.
Review of the Medical Literature
Here are key anchor points to the extensive scientific literature that establishes that wearing surgical masks and respirators (e.g., “N95”) does not reduce the risk of contracting a verified illness:
Jacobs, J. L. et al. (2009) “Use of surgical face masks to reduce the incidence of the common cold among health care workers in Japan: A randomized controlled trial”, American Journal of Infection Control, Volume 37, Issue 5, 417 – 419. https://www.ncbi.nlm.nih.gov/pubmed/19216002
N95-masked health-care workers (HCW) were significantly more likely to experience headaches. Face mask use in HCW was not demonstrated to provide benefit in terms of cold symptoms or getting colds.
Cowling, B. et al. (2010) “Face masks to prevent transmission of influenza virus: A systematic review”, Epidemiology and Infection, 138(4), 449-456. doi:10.1017/S0950268809991658
None of the studies reviewed showed a benefit from wearing a mask, in either HCW or community members in households (H). See summary Tables 1 and 2 therein.
bin-Reza et al. (2012) “The use of masks and respirators to prevent transmission of influenza: a systematic review of the scientific evidence”, Influenza and OtherRespiratory Viruses 6(4), 257–267. https://onlinelibrary.wiley.com/doi/epdf/10.1111/j.1750-2659.2011.00307.x
“There were 17 eligible studies. … None of the studies established a conclusive relationship between mask ⁄ respirator use and protection against influenza infection.”
Smith, J.D. et al. (2016) “Effectiveness of N95 respirators versus surgical masks in protecting health care workers from acute respiratory infection: a systematic review and meta-analysis”, CMAJ Mar 2016, cmaj.150835; DOI: 10.1503/cmaj.150835 https://www.cmaj.ca/content/188/8/567
“We identified 6 clinical studies … In the meta-analysis of the clinical studies, we found no significant difference between N95 respirators and surgical masks in associated risk of (a) laboratory-confirmed respiratory infection, (b) influenza-like illness, or (c) reported work-place absenteeism.”
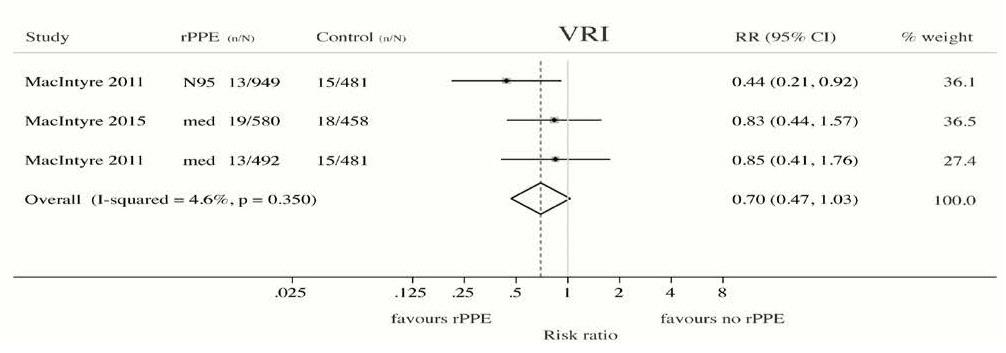
Offeddu, V. et al. (2017) “Effectiveness of Masks and Respirators Against Respiratory
Infections in Healthcare Workers: A Systematic Review and Meta-Analysis”, Clinical Infectious Diseases, Volume 65, Issue 11, 1 December 2017, Pages 1934–1942, https://doi.org/10.1093/cid/cix681
https://academic.oup.com/cid/article/65/11/1934/4068747
“Self-reported assessment of clinical outcomes was prone to bias. Evidence of a protective effect of masks or respirators against verified respiratory infection (VRI) was not statistically significant”; as per Fig. 2c therein:
Radonovich, L.J. et al. (2019) “N95 Respirators vs Medical Masks for Preventing Influenza Among Health Care Personnel: A Randomized Clinical Trial”, JAMA. 2019; 322(9): 824–833. doi:10.1001/jama.2019.11645 https://jamanetwork.com/journals/jama/fullarticle/2749214
“Among 2862 randomized participants, 2371 completed the study and accounted for 5180 HCW-seasons. … Among outpatient health care personnel, N95 respirators vs medical masks as worn by participants in this trial resulted in no significant difference in the incidence of laboratory-confirmed influenza.”
Long, Y. et al. (2020) “Effectiveness of N95 respirators versus surgical masks against
influenza: A systematic review and meta-analysis”, J Evid Based Med. 2020; 1- 9. https://doi.org/10.1111/jebm.12381 https://onlinelibrary.wiley.com/doi/epdf/10.1111/jebm.12381
“A total of six RCTs involving 9 171 participants were included. There were no statistically significant differences in preventing laboratory-confirmed influenza, laboratory-confirmed respiratory viral infections, laboratory-confirmed respiratory infection and influenza-like illness using N95 respirators and surgical masks. Meta-analysis indicated a protective effect of N95 respirators against laboratory-confirmed bacterial colonization (RR = 0.58, 95% CI 0.43-0.78). The use of N95 respirators compared with surgical masks is not associated with a lower risk of laboratory-confirmed influenza.”
Conclusion Regarding that Masks Do Not Work
No RCT study with verified outcome shows a benefit for HCW or community members in households to wearing a mask or respirator. There is no such study. There are no exceptions.
Likewise, no study exists that shows a benefit from a broad policy to wear masks in public (more on this below).
Furthermore, if there were any benefit to wearing a mask, because of the blocking power against droplets and aerosol particles, then there should be more benefit from wearing a respirator (N95) compared to a surgical mask, yet several large meta-analyses, and all the RCT, prove that there is no such relative benefit.
Masks and respirators do not work.
Precautionary Principle Turned on Its Head with Masks
In light of the medical research, therefore, it is difficult to understand why public-health authorities are not consistently adamant about this established scientific result, since the distributed psychological, economic and environmental harm from a broad recommendation to wear masks is significant, not to mention the unknown potential harm from concentration and distribution of pathogens on and from used masks. In this case, public authorities would be turning the precautionary principle on its head (see below).
Physics and Biology of Viral Respiratory Disease and of Why Masks Do Not Work
In order to understand why masks cannot possibly work, we must review established knowledge about viral respiratory diseases, the mechanism of seasonal variation of excess deaths from pneumonia and influenza, the aerosol mechanism of infectious disease transmission, the physics and chemistry of aerosols, and the mechanism of the so-called minimum-infective-dose.
In addition to pandemics that can occur anytime, in the temperate latitudes there is an extra burden of respiratory-disease mortality that is seasonal, and that is caused by viruses. For example, see the review of influenza by Paules and Subbarao (2017). This has been known for a long time, and the seasonal pattern is exceedingly regular.
For example, see Figure 1 of Viboud (2010), which has “Weekly time series of the ratio of deaths from pneumonia and influenza to all deaths, based on the 122 cities surveillance in the US (blue line). The red line represents the expected baseline ratio in the absence of influenza activity,” here:
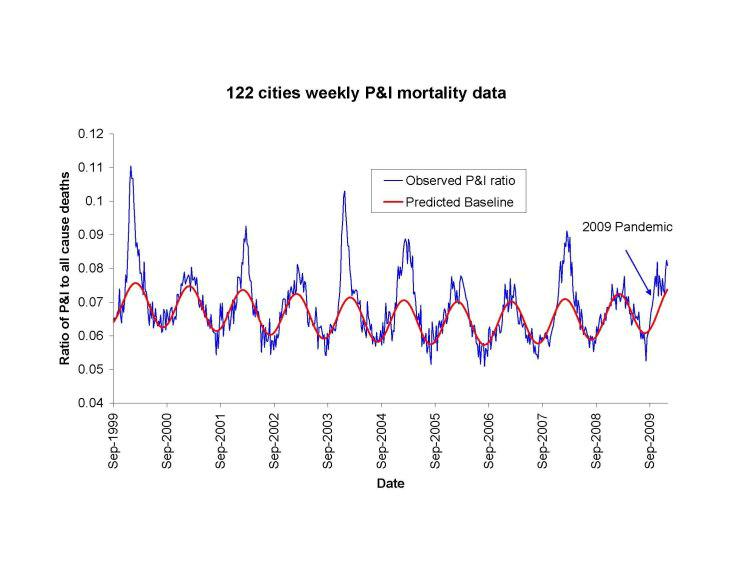
The seasonality of the phenomenon was largely not understood until a decade ago. Until recently, it was debated whether the pattern arose primarily because of seasonal change in virulence of the pathogens, or because of seasonal change in susceptibility of the host (such as from dry air causing tissue irritation, or diminished daylight causing vitamin deficiency or hormonal stress). For example, see Dowell (2001).
In a landmark study, Shaman et al. (2010) showed that the seasonal pattern of extra respiratory-disease mortality can be explained quantitatively on the sole basis of absolute humidity, and its direct controlling impact on transmission of airborne pathogens.
Lowen et al. (2007) demonstrated the phenomenon of humidity-dependent airborne-virus virulence in actual disease transmission between guinea pigs, and discussed potential underlying mechanisms for the measured controlling effect of humidity.
The underlying mechanism is that the pathogen-laden aerosol particles or droplets are neutralized within a half-life that monotonically and significantly decreases with increasing ambient humidity. This is based on the seminal work of Harper (1961). Harper experimentally showed that viral-pathogen-carrying droplets were inactivated within shorter and shorter times, as ambient humidity was increased.
Harper argued that the viruses themselves were made inoperative by the humidity (“viable decay”), however, he admitted that the effect could be from humidity-enhanced physical removal or sedimentation of the droplets (“physical loss”): “Aerosol viabilities reported in this paper are based on the ratio of virus titre to radioactive count in suspension and cloud samples, and can be criticized on the ground that test and tracer materials were not physically identical.”
The latter (“physical loss”) seems more plausible to me, since humidity would have a universal physical effect of causing particle / droplet growth and sedimentation, and all tested viral pathogens have essentially the same humidity-driven “decay”. Furthermore, it is difficult to understand how a virion (of all virus types) in a droplet would be molecularly or structurally attacked or damaged by an increase in ambient humidity. A “virion” is the complete, infective form of a virus outside a host cell, with a core of RNA or DNA and a capsid. The actual mechanism of such humidity-driven intra-droplet “viable decay” of a virion has not been explained or studied.
In any case, the explanation and model of Shaman et al. (2010) is not dependant on the particular mechanism of the humidity-driven decay of virions in aerosol / droplets. Shaman’s quantitatively demonstrated model of seasonal regional viral epidemiology is valid for either mechanism (or combination of mechanisms), whether “viable decay” or “physical loss”.
The breakthrough achieved by Shaman et al. is not merely some academic point. Rather, it has profound health-policy implications, which have been entirely ignored or overlooked in the current coronavirus pandemic.
In particular, Shaman’s work necessarily implies that, rather than being a fixed number (dependent solely on the spatial-temporal structure of social interactions in a completely susceptible population, and on the viral strain), the epidemic’s basic reproduction number (R0) is highly or predominantly dependent on ambient absolute humidity.
For a definition of R0, see HealthKnowlege-UK (2020): R0 is “the average number of secondary infections produced by a typical case of an infection in a population where everyone is susceptible.” The average R0 for influenza is said to be 1.28 (1.19–1.37); see the comprehensive review by Biggerstaff et al. (2014).
In fact, Shaman et al. showed that R0 must be understood to seasonally vary between humid-summer values of just larger than “1” and dry-winter values typically as large as “4” (for example, see their Table 2). In other words, the seasonal infectious viral respiratory diseases that plague temperate latitudes every year go from being intrinsically mildly contagious to virulently contagious, due simply to the bio-physical mode of transmission controlled by atmospheric humidity, irrespective of any other consideration.
Therefore, all the epidemiological mathematical modelling of the benefits of mediating policies (such as social distancing), which assumes humidity-independent R0 values, has a large likelihood of being of little value, on this basis alone. For studies about modelling and regarding mediation effects on the effective reproduction number, see Coburn (2009) and Tracht (2010).
To put it simply, the “second wave” of an epidemic is not a consequence of human sin regarding mask wearing and hand shaking. Rather, the “second wave” is an inescapable consequence of an air-dryness-driven many-fold increase in disease contagiousness, in a population that has not yet attained immunity.
If my view of the mechanism is correct (i.e., “physical loss”), then Shaman’s work further necessarily implies that the dryness-driven high transmissibility (large R0) arises from small aerosol particles fluidly suspended in the air; as opposed to large droplets that are quickly gravitationally removed from the air.
Such small aerosol particles fluidly suspended in air, of biological origin, are of every variety and are everywhere, including down to virion-sizes (Despres, 2012). It is not entirely unlikely that viruses can thereby be physically transported over inter-continental distances (e.g., Hammond, 1989).
More to the point, indoor airborne virus concentrations have been shown to exist (in day-care facilities, health centres, and onboard airplanes) primarily as aerosol particles of diameters smaller than 2.5 μm, such as in the work of Yang et al. (2011):
“Half of the 16 samples were positive, and their total virus concentrations ranged from 5800 to 37 000 genome copies m−3. On average, 64 per cent of the viral genome copies were associated with fine particles smaller than 2.5 µm, which can remain suspended for hours. Modelling of virus concentrations indoors suggested a source strength of 1.6 ± 1.2 × 105 genome copies m−3 air h−1 and a deposition flux onto surfaces of 13 ± 7 genome copies m−2 h−1 by Brownian motion. Over 1 hour, the inhalation dose was estimated to be 30 ± 18 median tissue culture infectious dose (TCID50), adequate to induce infection. These results provide quantitative support for the idea that the aerosol route could be an important mode of influenza transmission.”
Such small particles (< 2.5 μm) are part of air fluidity, are not subject to gravitational sedimentation, and would not be stopped by long-range inertial impact. This means that the slightest (even momentary) facial misfit of a mask or respirator renders the design filtration norm of the mask or respirator entirely irrelevant. In any case, the filtration material itself of N95 (average pore size ~0.3−0.5 μm) does not block virion penetration, not to mention surgical masks. For example, see Balazy et al. (2006).
Mask stoppage efficiency and host inhalation are only half of the equation, however, because the minimal infective dose (MID) must also be considered. For example, if a large number of pathogen-laden particles must be delivered to the lung within a certain time for the illness to take hold, then partial blocking by any mask or cloth can be enough to make a significant difference.
On the other hand, if the MID is amply surpassed by the virions carried in a single aerosol particle able to evade mask-capture, then the mask is of no practical utility, which is the case.
Yezli and Otter (2011), in their review of the MID, point out relevant features:
- most respiratory viruses are as infective in humans as in tissue culture having optimal laboratory susceptibility
- it is believed that a single virion can be enough to induce illness in the host
- the 50%-probability MID (“TCID50”) has variably been found to be in the range 100−1000 virions
- there are typically 103−107 virions per aerolized influenza droplet with diameter 1 μm − 10 μm
- the 50%-probability MID easily fits into a single (one) aerolized droplet
For further background:
- A classic description of dose-response assessment is provided by Haas (1993).
- Zwart et al. (2009) provided the first laboratory proof, in a virus-insect system, that the action of a single virion can be sufficient to cause disease.
- Baccam et al. (2006) calculated from empirical data that, with influenza A in humans, “we estimate that after a delay of ~6 h, infected cells begin producing influenza virus and continue to do so for ~5 h. The average lifetime of infected cells is ~11 h, and the half-life of free infectious virus is ~3 h. We calculated the [in-body] basic reproductive number, R0, which indicated that a single infected cell could produce ~22 new productive infections.”
- Brooke et al. (2013) showed that, contrary to prior modeling assumptions, although not all influenza-A-infected cells in the human body produce infectious progeny (virions), nonetheless, 90% of infected cell are significantly impacted, rather than simply surviving unharmed.
All of this to say that: if anything gets through (and it always does, irrespective of the mask), then you are going to be infected. Masks cannot possibly work. It is not surprising, therefore, that no bias-free study has ever found a benefit from wearing a mask or respirator in this application.
Therefore, the studies that show partial stopping power of masks, or that show that masks can capture many large droplets produced by a sneezing or coughing mask-wearer, in light of the above-described features of the problem, are irrelevant. For example, such studies as these: Leung (2020), Davies (2013), Lai (2012), and Sande (2008).
Why There Can Never Be an Empirical Test of a Nation-Wide Mask-Wearing Policy
As mentioned above, no study exists that shows a benefit from a broad policy to wear masks in public. There is good reason for this. It would be impossible to obtain unambiguous and bias-free results:
- Any benefit from mask-wearing would have to be a small effect, since undetected in controlled experiments, which would be swamped by the larger effects, notably the large effect from changing atmospheric humidity.
- Mask compliance and mask adjustment habits would be unknown.
- Mask-wearing is associated (correlated) with several other health behaviours; see Wada (2012).
- The results would not be transferable, because of differing cultural habits.
- Compliance is achieved by fear, and individuals can habituate to fear-based propaganda, and can have disparate basic responses.
- Monitoring and compliance measurement are near-impossible, and subject to large errors.
- Self-reporting (such as in surveys) is notoriously biased, because individuals have the self-interested belief that their efforts are useful.
- Progression of the epidemic is not verified with reliable tests on large population samples, and generally relies on non-representative hospital visits or admissions.
- Several different pathogens (viruses and strains of viruses) causing respiratory illness generally act together, in the same population and/or in individuals, and are not resolved, while having different epidemiological characteristics.
Unknown Aspects of Mask Wearing
Many potential harms may arise from broad public policies to wear masks, and the following unanswered questions arise:
- Do used and loaded masks become sources of enhanced transmission, for the wearer and others?
- Do masks become collectors and retainers of pathogens that the mask wearer would otherwise avoid when breathing without a mask?
- Are large droplets captured by a mask atomized or aerolized into breathable components? Can virions escape an evaporating droplet stuck to a mask fiber?
- What are the dangers of bacterial growth on a used and loaded mask?
- How do pathogen-laden droplets interact with environmental dust and aerosols captured on the mask?
- What are long-term health effects on HCW, such as headaches, arising from impeded breathing?
- Are there negative social consequences to a masked society?
- Are there negative psychological consequences to wearing a mask, as a fear-based behavioural modification?
- What are the environmental consequences of mask manufacturing and disposal?
- Do the masks shed fibres or substances that are harmful when inhaled?
Conclusion
By making mask-wearing recommendations and policies for the general public, or by expressly condoning the practice, governments have both ignored the scientific evidence and done the opposite of following the precautionary principle.
In an absence of knowledge, governments should not make policies that have a hypothetical potential to cause harm. The government has an onus barrier before it instigates a broad social-engineering intervention, or allows corporations to exploit fear-based sentiments.
Furthermore, individuals should know that there is no known benefit arising from wearing a mask in a viral respiratory illness epidemic, and that scientific studies have shown that any benefit must be residually small, compared to other and determinative factors.
Otherwise, what is the point of publicly funded science?
The present paper about masks illustrates the degree to which governments, the mainstream media, and institutional propagandists can decide to operate in a science vacuum, or select only incomplete science that serves their interests. Such recklessness is also certainly the case with the current global lockdown of over 1 billion people, an unprecedented experiment in medical and political history.
Endnotes:
Baccam, P. et al. (2006) “Kinetics of Influenza A Virus Infection in Humans”, Journal of Virology Jul 2006, 80 (15) 7590-7599; DOI: 10.1128/JVI.01623-05 https://jvi.asm.org/content/80/15/7590
Balazy et al. (2006) “Do N95 respirators provide 95% protection level against airborne viruses, and how adequate are surgical masks?”, American Journal of Infection Control, Volume 34, Issue 2, March 2006, Pages 51-57. doi:10.1016/j.ajic.2005.08.018 http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.488.4644&rep=rep1&type=pdf
Biggerstaff, M. et al. (2014) “Estimates of the reproduction number for seasonal, pandemic, and zoonotic influenza: a systematic review of the literature”, BMC Infect Dis 14, 480 (2014). https://doi.org/10.1186/1471-2334-14-480
Brooke, C. B. et al. (2013) “Most Influenza A Virions Fail To Express at Least One Essential Viral Protein”, Journal of Virology Feb 2013, 87 (6) 3155-3162; DOI: 10.1128/JVI.02284-12 https://jvi.asm.org/content/87/6/3155
Coburn, B. J. et al. (2009) “Modeling influenza epidemics and pandemics: insights into the future of swine flu (H1N1)”, BMC Med 7, 30. https://doi.org/10.1186/1741-7015-7-30
Davies, A. et al. (2013) “Testing the Efficacy of Homemade Masks: Would They Protect in an Influenza Pandemic?”, Disaster Medicine and Public Health Preparedness, Available on CJO 2013 doi:10.1017/dmp.2013.43 http://journals.cambridge.org/abstract_S1935789313000438
Despres, V. R. et al. (2012) “Primary biological aerosol particles in the atmosphere: a review”, Tellus B: Chemical and Physical Meteorology, 64:1, 15598, DOI: 10.3402/tellusb.v64i0.15598 https://doi.org/10.3402/tellusb.v64i0.15598
Dowell, S. F. (2001) “Seasonal variation in host susceptibility and cycles of certain infectious diseases”, Emerg Infect Dis. 2001;7(3):369–374. doi:10.3201/eid0703.010301 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2631809/
Hammond, G. W. et al. (1989) “Impact of Atmospheric Dispersion and Transport of Viral Aerosols on the Epidemiology of Influenza”, Reviews of Infectious Diseases, Volume 11, Issue 3, May 1989, Pages 494–497, https://doi.org/10.1093/clinids/11.3.494
Haas, C.N. et al. (1993) “Risk Assessment of Virus in Drinking Water”, Risk Analysis, 13: 545-552. doi:10.1111/j.1539-6924.1993.tb00013.x https://doi.org/10.1111/j.1539-6924.1993.tb00013.x
HealthKnowlege-UK (2020) “Charter 1a – Epidemiology: Epidemic theory (effective & basic reproduction numbers, epidemic thresholds) & techniques for analysis of infectious disease data (construction & use of epidemic curves, generation numbers, exceptional reporting & identification of significant clusters)”, HealthKnowledge.org.uk, accessed on 2020-04-10. https://www.healthknowledge.org.uk/public-health-textbook/research-methods/1a-epidemiology/epidemic-theory
Lai, A. C. K. et al. (2012) “Effectiveness of facemasks to reduce exposure hazards for airborne infections among general populations”, J. R. Soc. Interface. 9938–948 http://doi.org/10.1098/rsif.2011.0537
Leung, N.H.L. et al. (2020) “Respiratory virus shedding in exhaled breath and efficacy of face masks”, Nature Medicine (2020). https://doi.org/10.1038/s41591-020-0843-2
Lowen, A. C. et al. (2007) “Influenza Virus Transmission Is Dependent on Relative Humidity and Temperature”, PLoS Pathog 3(10): e151. https://doi.org/10.1371/journal.ppat.0030151
Paules, C. and Subbarao, S. (2017) “Influenza”, Lancet, Seminar| Volume 390, ISSUE 10095, P697-708, August 12, 2017. http://dx.doi.org/10.1016/S0140-6736(17)30129-0
Sande, van der, M. et al. (2008) “Professional and Home-Made Face Masks Reduce Exposure to Respiratory Infections among the General Population”, PLoS ONE 3(7): e2618. doi:10.1371/journal.pone.0002618 https://doi.org/10.1371/journal.pone.0002618
Shaman, J. et al. (2010) “Absolute Humidity and the Seasonal Onset of Influenza in the Continental United States”, PLoS Biol 8(2): e1000316. https://doi.org/10.1371/journal.pbio.1000316
Tracht, S. M. et al. (2010) “Mathematical Modeling of the Effectiveness of Facemasks in Reducing the Spread of Novel Influenza A (H1N1)”, PLoS ONE 5(2): e9018. doi:10.1371/journal.pone.0009018
https://doi.org/10.1371/journal.pone.0009018
Viboud C. et al. (2010) “Preliminary Estimates of Mortality and Years of Life Lost Associated with the 2009 A/H1N1 Pandemic in the US and Comparison with Past Influenza Seasons”, PLoS Curr. 2010; 2:RRN1153. Published 2010 Mar 20. doi:10.1371/currents.rrn1153 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2843747/
Wada, K. et al. (2012) “Wearing face masks in public during the influenza season may reflect other positive hygiene practices in Japan”, BMC Public Health 12, 1065 (2012). https://doi.org/10.1186/1471-2458-12-1065
Yang, W. et al. (2011) “Concentrations and size distributions of airborne influenza A viruses measured indoors at a health centre, a day-care centre and on aeroplanes”, Journal of the Royal Society, Interface. 2011 Aug;8(61):1176-1184. DOI: 10.1098/rsif.2010.0686. https://royalsocietypublishing.org/doi/10.1098/rsif.2010.0686
Yezli, S., Otter, J.A. (2011) “Minimum Infective Dose of the Major Human Respiratory and Enteric Viruses Transmitted Through Food and the Environment”, Food Environ Virol 3, 1–30. https://doi.org/10.1007/s12560-011-9056-7
Zwart, M. P. et al. (2009) “An experimental test of the independent action hypothesis in virus– insect pathosystems”, Proc. R. Soc. B. 2762233–2242 http://doi.org/10.1098/rspb.2009.0064

")


[…] must agree to receive a COVID vaccination or sign a “declination form” that would mandate “masking” indefinitely in addition to other castigatory […]